Scoring the Longevity Peptides: A Method for Not Fooling Yourself

There are roughly a dozen peptides on the market right now making some version of the same pitch: slow the clock, feel younger, live longer. The problem isn’t scarcity of options. It’s that the marketing volume and the evidence quality for these compounds don’t move together, and most people have no simple way to check one against the other before they spend money or put something under their skin.
This piece treats the question the way an analyst would treat any claim with a dollar sign attached to it: build a small, honest rubric, run each popular compound through it, and report what falls out, including the places where the method itself runs thin. Nothing here is a buy signal. It’s a way of reading the label more carefully than the label wants you to.
The rubric, up front
Four questions get asked of every compound before anything else matters:
- What specific outcome is being claimed (skin, energy, physical function, lifespan)?
- What is the best human evidence for that specific compound, doing that specific thing?
- Was that evidence a controlled human trial, an association, or an animal result?
- What dose did the strongest study actually use, versus what’s being sold?
None of this is exotic. It’s the same filter a careful reader would apply to any health claim. The value is in applying it consistently instead of letting the boldest claim get a pass because it’s the most exciting one.
Running the compounds through it
GHK-Cu (copper peptide), goal: skin. This is the strongest data point in the set for a specific, narrow claim. A 2018 review tracked GHK levels in blood declining with age, from about 200 nanograms per milliliter in someone’s twenties down to roughly 80 by age 60, and reported that topical GHK-Cu improved collagen production in about 70% of women studied, outperforming vitamin C and retinoic acid creams in those comparisons [3]. Score that data point high, but score it high specifically for topical, skin-level claims. The evidence was gathered from creams and patches on skin, not injections aimed at whole-body aging, and stretching a topical result into a systemic one is exactly the kind of leap this rubric exists to catch.
NMN, goal: physical function. This is the best-designed human trial in the category. A 2023 randomized, placebo-controlled study gave 80 healthy middle-aged adults 300, 600, or 900 mg of NMN daily for 60 days and found rising NAD+ levels alongside improved six-minute walk distance [1]. NAD+ is a coenzyme known to decline with age [2], so the mechanism has a logical backbone. Score the trial design high. But read the outcome column carefully: it measured NAD+ and a walking test over two months, not lifespan and not “anti-aging” as a general category. A compound can score well on trial rigor and still not support the biggest claim made about it.
SS-31 (elamipretide), goal: mitochondrial/longevity-adjacent. This one is instructive precisely because it did the hard thing and still came up short. It’s a mitochondrial peptide that went through an actual phase 3 trial (MMPOWER-3) in 218 people with primary mitochondrial myopathy, dosed at 40 mg a day, and it missed its primary endpoints against placebo [4]. On this rubric, SS-31 scores near the top for trial rigor and near the bottom for result. That combination, real trial, negative outcome, is rarer than it should be in this category, and worth taking seriously rather than explaining away.
Humanin, goal: lifespan. Genuinely interesting biology: it extends lifespan in C. elegans and runs elevated in the children of people who live past 100 [5]. But run it through question three and the honest label appears immediately: that’s an association in humans, not a trial of what happens when a person takes it. Score the underlying science as promising and the applied human evidence as effectively absent.
The pattern across all four is consistent enough to state as a working rule: the bigger the promise (lifespan over skin, systemic over topical), the thinner the human trial data tends to be. That’s not a cynical take, it’s what the citation trail actually shows when you follow it compound by compound.
Scoring the delivery method, not just the molecule
A compound’s evidence score is only half the picture. The other half is how it reaches you, and that variable moves the risk number more than people expect.
Two delivery models exist side by side. In one, a licensed clinician reviews your history and medications, decides whether a compound is appropriate, and a licensed pharmacy prepares it, with someone accountable if something goes wrong. In the other, a website has you check a “for research use only” box and ships a vial to your door, no intake, no clinician, no one responsible for whether the contents match the label.
Scored honestly, that second model doesn’t get partial credit. It fails on every column that matters for an experimental category: no one catches a drug interaction, no one flags that a particular compound is a bad idea for your specific situation, no one distinguishes the compounds with real trials from the ones running on hope. A vial with a sticker isn’t a cheaper version of medical oversight. It’s a different category of product wearing similar packaging.
For what a passing score on delivery actually looks like: a real intake about health and medications, a licensed clinician able to say no, a prescription when warranted, dispensing through a licensed pharmacy operating under recognized compounding standards, and a way to reach someone afterward. FormBlends is one example worth naming here, a physician-supervised telehealth service that routes these compounds through a clinician and a licensed 503A pharmacy rather than shipping unreviewed research chemicals, and that describes its products as compounded preparations rather than guaranteed cures. That’s mentioned once, as an illustration of what the passing model looks like in practice, not as an endorsement to buy anything. The oversight doesn’t upgrade an unproven compound to a proven one. It just means a qualified person is actually in the loop, which is a separate and real variable worth scoring on its own.
Where the dosing numbers actually come from
If a compound clears the evidence and oversight checks, the next thing worth scoring is the dose, because “more” is the instinct that gets people into trouble here.
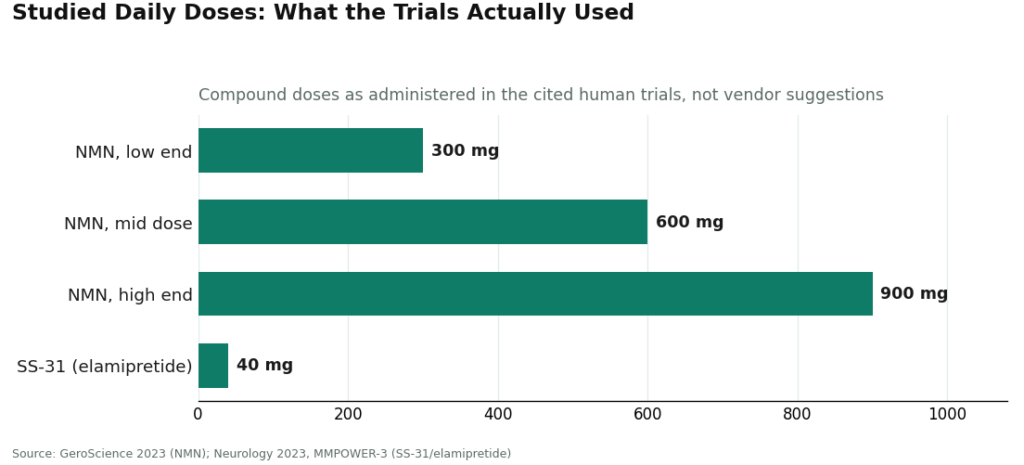
The trials give specific, knowable numbers, not round guesses. The NMN study used 300, 600, or 900 mg daily, with the strongest effects showing up at the higher end of that range [1]. SS-31’s phase 3 trial used 40 mg a day [4]. Those figures came out of controlled research, not a forum thread, and the responsible move is to anchor on them and let a clinician translate the number to an individual case, since none of us was actually in the trial population.
Pushing past the studied dose isn’t diligence, it’s an unblinded experiment on one person with no comparison group and no safety monitor. For most of these compounds, there’s no solid long-term safety data in healthy people taking them for anti-aging purposes, which argues for conservatism, not for chasing a bigger number.
Keeping a record matters here too, and it’s a low-cost way to raise the quality of your own data. Whatever gets taken, write down the what, the when, and what was actually noticed, including the weeks where nothing happened. A written log handed to a clinician is worth far more than a remembered impression of “I think it helped.” Some people use a structured tool for this, like the FormBlends tracker app, purely to log symptoms and timing over weeks, nothing more, no purchase attached to the logging itself. A notebook does the same job.
Where this method runs out of road
Any honest scorecard has to own its blind spots, and this one has several.
It can’t measure lifespan, because none of the underlying studies did. Nobody has completed a human trial that follows people for decades to see if a peptide extends life, and that gap doesn’t get smaller just because a product is marketed with lifespan language. This method can only score what was actually tested, which for most of these compounds is a much narrower thing than “anti-aging.”
It can’t fully close the animal-to-human gap. Humanin’s worm data is real, but a worm result doesn’t transfer with any predictable ratio to a human outcome, and this rubric has no way to convert one into the other. It can flag the gap. It can’t fill it.
It also can’t verify what a research-chemical vendor actually ships. A dosing number from a published trial tells you what was studied, not what’s in an unregulated vial, and the FDA’s 2026 warning letters made the point directly: labeling something “research use only” doesn’t exempt it from oversight if it’s being marketed for human use [6]. Purity and concentration are variables this scorecard simply can’t check from the outside, which is one more reason the oversight model matters as much as the molecule.
The final tally
Name the specific outcome wanted before naming a compound. Match that compound to its best human evidence, not its loudest claim, and expect the boldest promises to carry the thinnest data. Score the delivery model as seriously as the molecule: a clinician who can say no and a licensed pharmacy behind it beats a vial with a research-use sticker every time. Anchor any dose on what was actually studied, resist pushing past it, and keep a real log instead of a memory. Run the numbers this way and the decision stops being a bet on hype and starts being a documented, adult call, which is about as good as this category gets right now.
The compounds discussed are early-stage, compounded, or sold for laboratory research use only, and none is an FDA-approved anti-aging or longevity therapy. Dosing figures reflect what was used in published research, not a recommendation. Check with a licensed clinician before starting anything in this category.
Answers to the common questions
Which anti-aging peptide scores best on the evidence? There’s no single winner because “best” depends on what’s being measured. For skin specifically, GHK-Cu has the strongest human data, with topical studies showing improved collagen in roughly 70% of women [3]. For measurable physical function, NMN has the best-designed human trial, a 2023 randomized, placebo-controlled study where 300 to 900 mg daily raised NAD+ and improved six-minute walk distance over 60 days [1]. Neither trial measured lifespan, because neither was built to. As a rule, the compounds marketed hardest on lifespan tend to score lowest on human evidence.
Has anything actually been shown to extend human lifespan? Not in a trial, no. That study is enormously difficult to run and nobody has completed one. Humanin extends lifespan in worms and shows up elevated in the children of centenarians, but that’s an association in humans, not evidence that taking it does anything [5]. A lifespan claim on a label should be read as the weakest-evidenced claim in the category, not the strongest.
SS-31 had serious hype behind it. Why did it fail? Because it was actually tested rigorously, and the test came back negative. SS-31 (elamipretide) went through a real phase 3 trial in people with primary mitochondrial myopathy, dosed at 40 mg a day, and didn’t beat placebo on its primary measures [4]. It’s a useful data point precisely because it’s one of the few cases in this space where a compelling mechanism got a genuine human trial, and the story that came out the other side was a miss.
How do you tell a legitimate provider from a research-chemical vendor? Look for a real health and medication intake, a licensed clinician who can decline to prescribe, an actual prescription when warranted, dispensing through a licensed pharmacy under recognized compounding standards, and a way to reach someone afterward. A research-chemical site skips all of it, letting a vial go into a cart under a “research use only” label with nobody accountable for whether the contents match what’s on it. The FDA’s 2026 warning letters specifically called out that labeling pattern as insufficient when a product is marketed for human use [6].
What dose should someone actually use? Anchor on the dose from the actual trial for that specific compound, then let a clinician scale it to the individual, since nobody was literally in the study population. The NMN trial used 300 to 900 mg daily with the strongest effects at the top of that range [1], and SS-31 was studied at 40 mg a day [4]. The instinct to go higher than the trial should be resisted, since long-term safety data in healthy people using these for anti-aging purposes is largely absent.
Does going through a clinician make an unproven compound proven? No, and that distinction matters. Clinician and pharmacy oversight adds real accountability, someone able to catch an interaction or flag a bad fit for a given person, but it doesn’t change what the underlying trials actually showed. The evidence score and the oversight score are two separate columns, and neither substitutes for the other.
Do peptides for anti-aging actually work, or is it mostly hype?
Scored honestly, some peptides carry real if modest evidence and others are close to pure speculation. Topical peptides like matrixyl (palmitoyl pentapeptide-4) have small, reasonably solid studies showing improvement in fine lines. Injectables like BPC-157 or epithalon have interesting animal data, but human trials are sparse and often underpowered. Read across the whole set and the fair conclusion is that the field is promising but still young, which should set expectations accordingly.
Are peptides for anti-aging safe to use?
Safety splits almost entirely along which peptide, what dose, what source, and how it’s administered. Well-studied topical peptides sold in cosmetics carry a low risk profile for most people. Injectable peptides bought from research-chemical suppliers sit in a different risk tier entirely, since purity, sterility, and dosing accuracy are rarely guaranteed there. Physician-supervised compounding pharmacies, FormBlends among them, operate under accountability standards that unregulated vendors simply don’t carry, and that gap matters a great deal when the product in question is going under the skin.
What are the best peptides for anti-aging based on current evidence?
No compound wins across every goal on this scorecard, but a few post better numbers than the rest. Oral collagen peptides have several small randomized trials showing skin hydration and elasticity benefits. Topical copper peptides and matrixyl-family compounds carry decent cosmetic-grade evidence. GHK-Cu shows up in a lot of respected research, though mostly at the in-vitro level. Injectable options like sermorelin come out of established endocrine medicine, though anti-aging use specifically remains off-label with limited long-term safety data behind it.
Where should someone actually buy peptides for anti-aging without getting burned?
The source matters as much as the compound. For topicals, established skincare brands with published formulation data are a reasonable starting point. For injectables, the only route with real accountability built in is a licensed prescribing physician working with a regulated compounding pharmacy, since that path comes with third-party testing records and medical oversight attached. Buying injectables from unregulated online vendors under a “research use only” label leaves no reliable way to check purity, concentration, or sterility.
References
- NMN randomized, placebo-controlled, dose-dependent trial: 300 to 900 mg daily in 80 healthy middle-aged adults raised NAD+ and improved six-minute walk distance over 60 days. GeroScience, 2023. https://pubmed.ncbi.nlm.nih.gov/36482258/
- NAD+ declines with age and that depletion is tied to aging-related diseases; review of NAD+ precursors including NMN. Biochemical and Biophysical Research Communications, 2024. https://pubmed.ncbi.nlm.nih.gov/38340651/
- GHK-Cu copper peptide review: plasma GHK declines from ~200 to ~80 ng/mL with age; topical GHK-Cu improved collagen in ~70% of women in skin studies. Pickart and Margolina, International Journal of Molecular Sciences, 2018.
- MMPOWER-3 phase 3 trial of elamipretide (SS-31), 40 mg/day in 218 people with primary mitochondrial myopathy; primary endpoints not met. Neurology, 2023.
- Mitochondrial-derived peptide humanin as a regulator of lifespan and healthspan: lifespan extension in C. elegans, elevated in centenarians’ offspring; largely preclinical, human data is association. Aging, 2020.
- FDA warning letters to research-peptide sellers; “research use only” labeling does not exempt products marketed for human use. FDA, dated March 31, 2026.
Written by Wren Zamora, health-data reporter. Reading the studies before believing the pitch. Last reviewed February 2026.
Educational material only. A licensed provider should evaluate your situation before you act.